Right now, more than 830 wildfires are burning across Canada. Canadian wildfire smoke is crossing the Great Lakes and reaching New England, with air quality alerts active across dozens of North American cities. For most people, wildfire smoke means closing windows and checking an app. For clinical teams responsible for embryos, surgical patients, senior residents, and vulnerable populations, it means something more immediate — and more difficult to manage than most facilities realize.
The challenge is not visible. Inside most clinical buildings, you cannot smell Canadian wildfire smoke. You cannot see it. But it is there, and the filtration systems most facilities rely on were not designed to stop the most dangerous part of it.
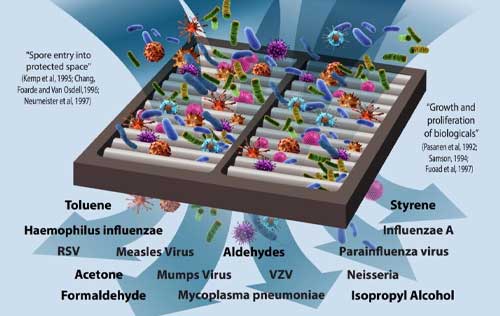
Wildfire smoke is a complex mixture. Three categories matter in clinical environments:
Particulates — fine and ultrafine particles including PM2.5 and smaller. HEPA filtration captures a portion of these within its designed size range.
Volatile organic compounds (VOCs) — combustion-derived chemicals including formaldehyde, benzene, acrolein, and toluene. These are molecular-level contaminants that pass through HEPA filtration entirely, at concentrations far below what the human nose detects.
Gases — including carbon monoxide and other combustion products. Standard building filtration does not address these.

Canadian wildfire smoke penetrates buildings rapidly — standard HVAC systems pull outdoor air in continuously, bringing smoke-derived chemicals directly into the occupied space.
VOC concentrations inside buildings during wildfire events can exceed outdoor levels in some cases due to off-gassing from surfaces that have absorbed contamination.
PM2.5 from wildfire smoke is significantly more toxic per unit than PM2.5 from other sources, due to its specific chemical composition.
Wildfire smoke VOCs include known carcinogens and reproductive toxins — the same chemical families that IVF research has documented as harmful to embryo development at parts-per-billion concentrations.
HEPA filters capture particles. They do not capture VOCs, gases, or the chemical contamination that represents the primary threat from wildfire smoke in sensitive clinical environments.
A wildfire does not need to be nearby to affect indoor air quality. Canadian wildfire smoke from fires hundreds of miles away can produce hazardous conditions in cities with otherwise excellent air quality — as Toronto experienced throughout summer 2025 and is experiencing again in 2026.
The human embryo is the most air-quality-sensitive biological entity in clinical medicine. VOCs at parts-per-billion concentrations — documented in peer-reviewed research published in Reproductive BioMedicine Online and Fertility and Sterility — measurably impair cell division, disrupt embryo morphokinetics, and reduce pregnancy rates. There is no safe threshold for combustion-derived VOC exposure in the embryo culture environment.
Surgical and recovering hospital patients are already under immune system stress. Adding airborne chemical burden from wildfire smoke to a recovery environment slows healing and increases physiological load — across the entire patient census, not just the patients who develop a diagnosable infection.
Senior residents in long-term care and memory support have both higher continuous exposure (they live in the facility) and lower physiological reserve to manage chemical irritants. During a Canadian wildfire smoke event, the cumulative chemical burden they absorb is substantially greater than any short-stay patient.
NICU and pediatric patients have developing immune systems and respiratory tracts that are particularly sensitive to chemical irritants. The NICU is often technically sophisticated — but the air feeding that environment travels through the same building infrastructure as the rest of the facility.
Clinical staff — nurses, embryologists, surgeons, care aides — accumulate full-shift exposure over consecutive days. Staff in facilities without adequate VOC remediation during wildfire events experience occupational chemical exposure that is real, measurable, and almost never discussed in wildfire health advisories.

HEPA is a capture strategy, not a purification strategy. It traps particles on a filter medium — it does not kill biological organisms or neutralize chemical contamination.
HEPA H13 standard captures 99.97% of particles above 0.3 microns. Wildfire smoke VOCs are molecular-level — orders of magnitude smaller than HEPA’s capture threshold.
A clinical facility relying solely on HEPA during a wildfire event is managing the smoke’s particulate component and leaving its chemical component entirely unaddressed.
The VOC content of wildfire smoke — formaldehyde, benzene, acrolein — is precisely the contamination category most threatening to embryos, recovering patients, and senior residents, and the category that HEPA was never designed to stop.
Increasing HVAC air change rates during a wildfire event does not solve the VOC problem — it accelerates the introduction of contaminated outdoor air into the building.
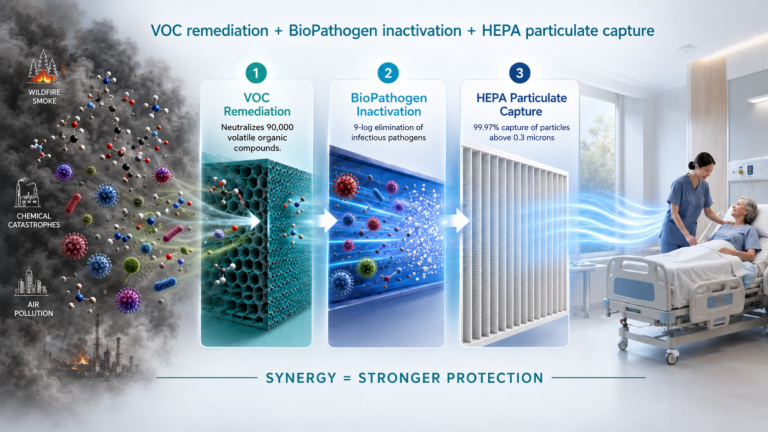
LifeAire’s multi-stage technology combines three protective mechanisms in a single pass through the system:
Every unit of air is treated before it reaches the protected clinical space. The system operates continuously — 24 hours a day, seven days a week — regardless of outdoor air quality conditions. There is no between-cycle interval during which the space is unprotected.
Facilities with LifeAire installed do not smell wildfire smoke inside the protected space. Clinical teams across LifeAire’s installed base are reporting this to us right now, during this active wildfire season.
During the 2025 Canadian wildfire season, when smoke from fires burning across Ontario pushed Toronto’s air quality into hazardous territory for weeks at a time, Christine S. Yeh, former Laboratory Director at Twig Fertility, documented what protection looked like in practice:
“Throughout the wildfire season, our LifeAire-protected laboratory maintained excellent air quality — with no detectable impact on embryo development or quality despite the severe external conditions. Having a robust air purification system in place provides confidence that, even when outside air quality is compromised, we can continue to deliver the highest standard of care for our patients and give every embryo the best possible opportunity to thrive.”
Christine S. Yeh, Former Laboratory Director
Twig Fertility, Toronto
“About a block to the south of us a restaurant had a fire…You could see the big plumes of smoke. This is a very scary thing. An unanticipated problem that could have dramatically affected our results and yet it did not because we have this system in place. The air from the LifeAire system was completely clean and pristine.”
Dr. Randy Morris, Medical Director
Naperville Fertility Center
The Aire~IRMU is available now for facilities needing immediate supplemental protection during an active Canadian wildfire smoke event. For a longer-term evaluation, the Aire~Analysis air quality assessment establishes a baseline VOC and pathogen measurement in your specific environment — the factual foundation for a confident investment decision.
Contact the LifeAire team to discuss your concerns and paths you can take to improve any airborne strategy.
Request an air quality assessment of your facility.
Read our published clinical research.
Learn how LifeAire and HEPA work together.
Learn about our pure air guarantee.
Read our guide about LifeAire’s role as an Infection Control Platform.
LifeAire was founded because the most vulnerable biological processes in clinical medicine deserved better air than standard filtration could provide. That remains the mission — in every season, and especially in this one.